-
Rest Pause
-
Load Drop Sets
-
Mechanical Drop Sets
-
Partial Reps
-
Myoreps
-
Cluster Sets
-
Forced Reps
-
Eccentrics
-
Self-Spotting
-
Alternating Reps
-
Marathon Sets
-
2 Up/1 Down Reps
-
Eccentric Quasi-Isometrics (EQIs)
-
Isoholds
-
Isometrics
-
Continuous Reps
-
Potentiation Sets
-
Ladders
-
Loaded Stretching
-
Blood Flow Restriction (Occlusion Training)
-
Against Blood-Flow Restriction
-
Pre-Exhausting
-
Banding & Reverse Banding (Accommodating Resistance)
-
Top Set/Down Set Training
Participants 458

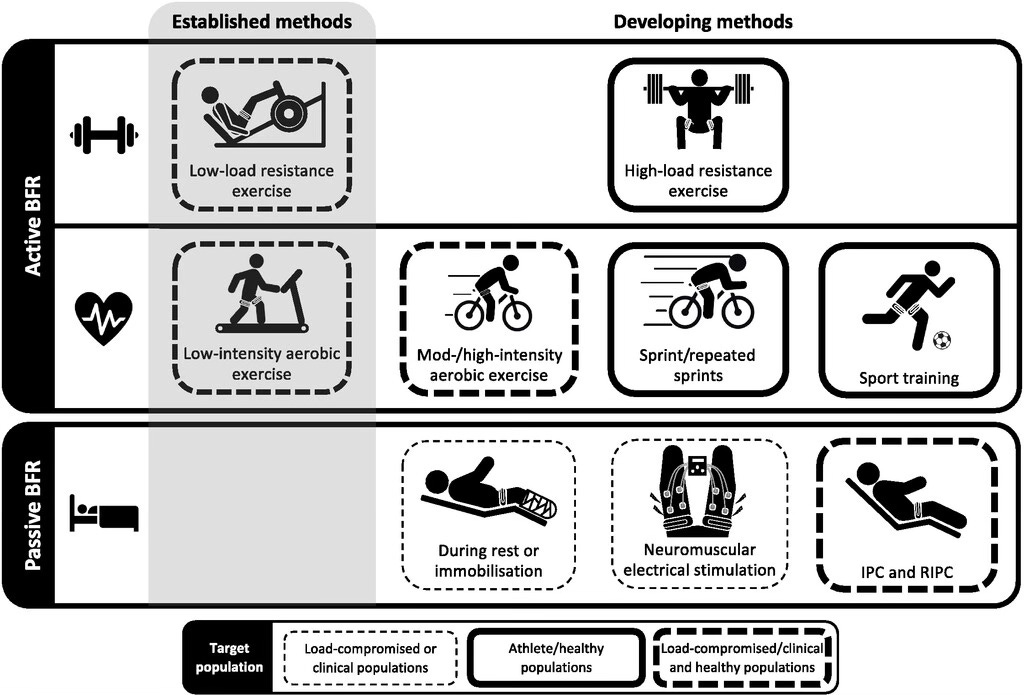
In a previous post, I detailed the effects of blood-flow restriction training and how to use it as a technique for promoting hypertrophy (or preventing atrophy).
As soon as I hit “Send”, I knew I was going to get shit for not emphasizing strongly enough the risks, caveats and contraindications.
So let’s flip-the-script today and steel-man the case against BFR…
But First, A Refresher
Blood-flow restriction (occlusion training) is a way to trap blood in a working muscle. The idea is to use some sort of occlusion device (i.e. elastic wrap, tourniquet, pressure wrap, etc) to compress the muscle proximally, which — when done right — will allow arterial inflows but prevent venous return. This creates an oxygen-deprived local environment and accumulates metabolites of contraction — both of which up-regulate the recruitment of anaerobic fibers (e.g. Type 2) as well as anabolic paracrine+autocrine signaling. Pooling of fluid forcibly expands the muscle’s volume — both within the individual sarcomeres (i.e. cell swelling) and surrounding them (e.g. interstitial space).
The clinically observed effects of BFR show some really interesting (and somewhat mysterious) things that happens with the above conditions:
First, atrophy can be held at bay without the need for external loading (Wengle et al, 2022) — This could be a Godsend for bedridden patients and those recovering from injury.
Second, hypertrophy can occur independently from progressive overload (Loenneke et al, 2012) — I know just thinking about this makes some people squirm, but the implications are pretty crazy. If we’re able to make gains from low-load training, it forces us to rethink the way we view the mechanisms of hypertrophy. And if we’re able to easily slot BFR into an already well-built, overloading program, it may offer the opportunity to pick some low-hanging, hypertrophic fruit.
Third, neural adaptations happen with BFR which are unique compared to high-load training (Centner et al, 2020) — We want our nervous system (central and peripheral) to be resilient enough to withstand traumatic events and plastic enough to make beneficial adaptations when called for. If BFR can be effective across a wide spectrum of neural use-cases (from retaining motor control post injury to preferential fiber-type conversion), it can be an incredibly valuable and versatile tool.
Fourth, performance markers can improve (e.g. strength, sprint time, agility tests, jump measurements) without specific training (Wortman et al, 2021) — This one just seems absurd to me so I won’t even attempt to pontificate on it. But imagine being able to increase your max vertical by doing occluded treadmill walking…just wtf?!
Risks and Other Bad Stuff
I want to use this moment to acknowledge my biases — clearly, I’m a proponent of the intelligent, strategic, and proper use of BFR. I’ve used it myself for years and seen awesome effects. My clients have used it for years and seen awesome effects. I’m probably a bit more laissez-faire about communicating the potential risks than I should be when discussing BFR. There’s also a high likelihood that this lackadaisical attitude is clouded by myself being (generally) healthy, my clients being (generally) healthy, and never having personally seen the consequences of BFR-gone-wrong.
So with all of that being said — with my biases on the table right next to all the rose-tinted benefits backed by my cherry-picked studies — I want to now do my best to present the most unbiased case possible AGAINST using blood-flow restriction.
- Venous Thromboembolism (i.e. blood clots) — This is as serious of a medical risk-vector as you’ll be able to find. With the disruption of normal blood flow as well as the pooling of blood, the chance of clot formation increases. Additionally, the pressure from the occlusion can damage and/or collapse vascular structures, leading to all sorts of issues (Nascimento et al, 2022). Additionally additionally, the populations who are at the greatest risk of developing VT (outside of genetic factors) tend to be those who are, in some way, immobilized; and as we discussed above, the prevention of atrophy in immobilized patients is one of the primary benefits of BFR. This is walking a tight-rope.
- Nerve Damage — The tight-rope act extends beyond vascularity and can be problematic for peripheral nerves as well. Too much pressure from BFR bands/straps/cuffs can compress the nerves running through the area, leading to acute (numbness, tingling, etc) or even chronic issues (pain, muscular weakness, etc) (Masri et al, 2020). This is one of the crucial reasons why it’s so important to get the occlusion pressure right; unfortunately, this is also the area where there is the most confusion and user-error (especially when being done with rudimentary straps and without supervision).
- Muscle Damage — Anyone who has ever tried BFR can attest to the unholy DOMs that accompany the technique. On its own, muscle damage isn’t a good or bad thing. It’s usually a decent proxy for sufficient hypertrophy stimuli (at the lower bounds) and recovery capacity (at the upper bounds). Muscle damage can also be brought on by the novelty effect, which is probably the source of most of BFR-related DOMs. And while adaptations to novelty (and occlusion training in particular) happen quickly, there is still the risk of overdoing it and causing downstream issues.
- Unknown Unknowns — There’s no way to hand-waive the fact that we still have a LOT to learn about the risks associated with BFR, over the short and long term. To be frank, we still have a lot to learn about the reasons why BFR even works. So any program designed to utilize this technique needs to account for externalities that are somewhat unpredictable.
Who Should Be Most Concerned About The Risks and Other Bad Stuff?
BFR isn’t going to be for all populations. Some people need to approach it with caution, perform it only under direct supervision, or even completely avoid it:
- Pre-existing Conditions — Those with a history of deep-vein thrombosis (DVT) or vascular disease shouldn’t use BFR. Those with diabetes, hypertension, or impaired blood coagulability should probably steer clear as well. Even pregnancy, rheumatoid arthritis, and PED-use can compound health risks. For these groups, as well as others that I haven’t listed, the risks of BFR can outweigh the gains, which is why it’s crucial to do your own research and talk to a doctor or professional before integrating any exercise strategy/technique (not just BFR).
- Training Age — Moving beyond clinical use-cases, the point of my original article was to discuss BFR as an alternative technique for inducing hypertrophy in healthy trainees. I contend that this is still a relevant use-case! However, those who have no need to implement it probably shouldn’t. And those who aren’t skilled/aware enough to adhere to the parameters of proper-use probably shouldn’t try. In other words, occlusion is an advanced technique for muscle growth and should only be used in this way by advanced athletes.
- Biological Age — Technically, biological age would classify as a pre-existing condition, but it’s worth filtering it out and addressing it independently. Old age brings with it tons of co-morbidities that are contraindicated with BFR; many of which we’ve already noted. While not a preclusion to BFR in and of itself, older adults need to be extremely cautious and follow their doctor’s prescriptions.
Considerations for Application
For most training techniques, the margin of error is relatively broad; if you make a mistake but land in the vicinity, it’s probably not going to dampen the desired effect too much. For BFR to be effective, you need a ringer; or at least, the horseshoe needs to be touching the stake. And there are A LOT of ways to fuck up the application and use of BFR:
- Occlusion Pressure — This is, by far, the most challenging aspect of the technique. In the clinical setting, there are calibrated, computer-controlled, pressurized cuffs that can be precisely adjusted to the micro-PSI. In the gym, we’re not so lucky. There’s been a recent surge of publicly available and affordable, state-of-the-art cuffs that can be controlled via an app, but I don’t have enough experience with these products to give a definitive review. Historically, simple elastic bands (i.e. knee wraps, wrist wraps, adjustable Velcro straps, etc) have been used to modulate the occlusion pressure. For trainees who understand what they’re doing and the proper tightness to shoot for, this was a sufficient though imperfect solution to create the desired effect. But most trainees who will be interested in using BFR aren’t going to fully grasp these best practices. Too loose and the blood can escape the working muscle. Too tight and the arterial flow is cut-off (plus the host of other issues that come with too much compression, which we’ve already discussed).
- Specificity of Target Muscles — I’m not sure why this is such a difficult concept for some people to grasp, but I continuously see the mistake of trying to target proximal muscles with a distal occlusion. Despite certain studies which show some interesting effects to the contrary (Bowman et al, 2019), BFR should be used as a primary technique ONLY for muscles that can be occluded proximally. This prerequisite includes the calves, quads, hamstrings, biceps, triceps, etc. This prerequisite excludes the glutes, delts, pecs, etc. So even though wrapping BFR bands around your thighs and performing high rep hip thrusts makes your glutes look ridiculous, the glutes aren’t actually the beneficiaries of the effect (ironically enough, the quads and hamstrings are in this example).
- Volume, Intensity, Frequency, and Fitting BFR Into Programming — There are BFR protocols for low-loads and high-loads. I’ve seen exact rep schemes (e.g. 30/15/15/15) and I’ve seen prescriptions for total-occlusion-time (i.e. 10 minutes of wrapped walking). I’ve seen BFR used in conjunction with bodybuilding, powerlifting, sport-specific training, and injury rehab. Sometimes it’s used as a stand-alone strategy, and other times it’s used in conjunction with more traditional resistance training methods. I’ve even personally built the use of BFR into a periodized model to try and take advantage of the metabolic/novelty effects while covering for the rapid desensitization that occurs in healthy, trained athletes. Just one glance at the breadth of the benefits should immediately tell you that there is an equally broad pool of potential applications and strategies of BFR. But there is no free lunch when it comes to physiology (write that down), and any use of BFR will come with its own specific trade-offs. Practically all protocols call for high volumes and high intensities (as a proxy for muscular failure). Most of the interesting ones utilize low relative loads. Frequency of use can vary significantly, and this gets even more convoluted when distinguishing between BFR use for a specific muscle versus any muscle. (In other words, how often you use BFR for your biceps will be different from how often you can use it for your biceps, triceps, quads, calves, etc). And then on top of all of these contingencies, you have to figure out the best way to integrate a relatively minor technique (in the grand scheme of things) into your broader programming without causing significant disruption. Obviously, this is all easier said than done.
- Subjective Feedback — As much as we all love to look at hard data, sometimes the best indicators come from subjective experience. The most sophisticated monitoring device ever created is the human body. Make sure to listen if it’s blasting you with physiological stop-signs.
Wrapping Up
Alright, I hope this quickly-thrown-together, extremely-partisan, probably-missing-key-arguments breakdown was at least good enough to reassure everyone that I do, in fact, think about the risks of blood-flow restriction even though I’m also a bro and like getting sick pumps.
If there way anything that I glaringly overlooked or didn’t do a good-enough job at explaining, please let me know so I can make corrections and present a more complete picture of the risks/benefits of BFR.